Absence of Coronary Disease – Can this be really true?
We have a global epidemic of chronic lifestyle diseases including cardiovascular disease with roughly 20 million deaths each year from coronary events and stroke. In the US alone, there is a coronary event every 34 seconds and a coronary event related death every minute and a half despite being an industrialized nation with the most advanced medical technology. These are scary and grim statistics. However, despite this gloom, we have now learned about the almost complete absence of cardiovascular disease in multiple contemporary populations around the globe. In this article, I have chronicled these tribes in an effort to learn what they do differently or are they blessed with a longevity gene.
We now know that 90% of cardiovascular disease can be attributed to conventional risk factors such as physical inactivity, increased body weight, sedentary lifestyle, high blood pressure, high cholesterol, smoking, and diabetes from large scale epidemiological studies such as the Framingham study (Dawber et al, Am J of Pub Health 1951), the Multi-Ethnic study of Atherosclerosis, MESA (Bild et al.Am J Epidemiol 2002), and the INTERHEART study (Yusuf et al. Lancet 2004). Populations which have not adopted a modern industrialized lifestyle are likely to have lower prevalence of the above mentioned risk factors and are the subject of this articles discussion.
In the Melanesian island of Papua New Guinea (Figure 1), a tribe of Kitava men and women, were assessed for prevalence of cardiovascular disease. There diet closely resembles the diet of our prehistoric human ancestors and is largely devoid of dairy products, cooking fat, sugar, cereals, alcohol, and salt. Lindeberg and Lundh (J Int Med 1993) studied 2250 Kitava inhabitants surviving on a healthy plant based diet. The main diet consists of cultivated tubers (mainly yam, sweet potato and taro), providing 50-70% of the diet, supplemented by fruits (banana, papaya, mango, watermelon, pineapple, guava, pumpkin), leaves, coconuts, fish, maize, tapioca, and beans. The basic utilities which we take for granted such as electricity, telephones and motor vehicles are absent. They do not suffer from diseases such as stroke, congestive heart failure, obesity, diabetes, ischemic heart disease, cancer, and even conditions such as acne. The commonest cause of death is infections and trauma. They have somewhat more physical activity compared to westerners but have strong social structure. The basic theme is that these individuals are not sedentary, eat largely a plant based diet, and have strong social bondage.
Figure 1 – Printed with permission – GNU Free Documentation License Ver 1.2

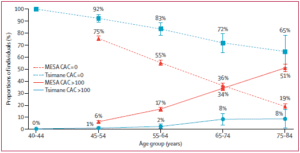
Another population which is of interest is the indigenous Tsimane tribe of Bolivia, a population of 16,000 that has a predominant lifestyle of hunting-gathering, and farming along the Maniqui river, an Amazon river tributary (Kaplan H et al, Lancet 2017). This tribe has low levels of high blood pressure and diabetes and are extremely physically active. A meticulous search for coronary atherosclerosis was performed in 705 Tsimane adults, using computed tomography (CT) to quantify the extent, severity, and location of coronary artery calcification (CAC). The mean age of the population studied was 57.6 years (41-92 years) and 50% of the participants were women. The Tsimane CAC scores were compared with the scores of other population-based studies in high income countries including the United States MESA study score. An individual with a CAC score above 100 is considered to be at higher risk for coronary atherosclerosis or coronary heart disease. A very low prevalence of coronary atherosclerosis was measured using the CAC score, with only 3% of the Tsimane population having a CAC score above 100 as compared to 50% of the MESA population with CAC above 100, making the Tsimane population with the lowest level of coronary atherosclerosis. In fact, the Tsimane men had even lower CAC values than even the Japanese women, a population having the lowest coronary risk of the industrialized nations. Figure 2 shows the percentage of CAC both below and above 100 across age groups in the Tsimane and MESA populations. In practical terms, a 80 year old Tsimane adult has a vascular age similar to a 50 year old American adult.
Figure 2: Coronary Artery Calcium Scores by age for US MESA, and Tsimane samples, MESA – Multi-Ethnic Study of Atherosclerosis.
Figure 3 – Tsimane Diet of Plantains.

This likely is the result of their lifestyle of physical activity and diet. The Tsimane diet lacks trans fat, and is a low fat diet, with an estimated daily consumption of 38 g fat, with 11 g saturated fat, 14 g monounsaturated fat, and 8 g polyunsaturated fat. An estimated 14% of their average caloric diet is protein, 14% is fat, and 72% is carbohydrates. Meat protein and fat are acquired by hunting and fresh water fishing. The non-processed carbohydrates are in the form of rice, plantain, manioc, and corn and also wild nuts and fruits (Figure 3). It is high in fiber and low in saturated fats and simple sugars. Moreover, less than 10% of their waking hours are spent in sedentary activity, as compared to more than 50% of sedentary time spent in industrialized nations.
Coronary atherosclerosis is the build-up of plaque in the arteries leading to the heart, which slows the blood flow and can cause blood clots – which may in turn lead to a heart attack. The researchers found that almost nine out of 10 of the 705 Tsimane adults who took part in the study had no risk at all of heart disease; 13% had a low risk and only 3% – 20 individuals – had moderate or high risk. Even in old age, 65% of those aged over 75 had almost no risk and only 8% (four out of 48) had a moderate to high risk. By contrast, in the US, a study of more than 6,800 people (MESA) found that half had moderate to high risk – five times as many as among the Tsimane people – and only 14% had no risk of heart disease at all.
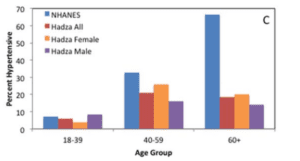
Another modern hunter-gatherer tribe called the “Hadza” live in northern Tanzania numbering around 2200 and follow a traditional lifestyle untouched by western lifestyle and industrialization (Figure 4). There lifestyle involves daily foraging for survival translating into a major amount of their time spent in moderate to vigorous physical activity. Raichlen and colleagues ( Am J Hum Biol. 2017) measured the physical activity of the Hadza using heart rate monitors and determined that the Hadza engage in over 14 times as much physical activity compared to individuals in the United States. Current guidelines recommend at least 150 min per week of moderate intensity activity or 75 min per week of vigorous intensity activity to improve cardiovascular health. A large accelerometry dataset from the National Health and Nutrition Examination Survey (NHANES), found that a geographically diverse sample of adults living in the United States engage in, on average, 45 min/week of moderate physical activity and 18 min/week of vigorous physical activity (i.e., just over an hour per week of moderate to vigorous physical activity) (Tucker et al. 2011). By comparison, the Raichlen et al (2017) data suggest Hadza participants engage in 805 min/week of moderate physical activity and 137 min/week of vigorousphysical activity, 14.8 times higher than adults in the US. Raichlen’s group also found almost complete absence of cardiovascular disease with low prevalence of hypertension (Figure 5) and optimal levels of cardiac bio-markers such as C-reactive protein, a marker of inflammation and cholesterol levels.
Figure 4 (With Permission) The Hadza Tribe Members Starting a Fire.

Figure 5 – Prevalence of hypertension by age in the Hadza participants compared with data from the U.S. (NHANES; Ong et al., 2007).
The Hadza diet is largely a plant based diet of wild berries, honey, fiber rich tubers, and some meat. One interesting study by Smits and colleagues (Nature 2017) documents the change in the Hadza intestinal microbiome which mirrors their changing seasonal food patterns. They analyzed 350 stool samples from Hadza people taken over the course of a year. They found that the intestinal bacteria found in Hadza is similar to seventeen other cultures around the world, which have similar lifestyles such as the hunter-gatherer communities in Venezuela and Peru and subsistence farmers in Malawi and Cameroon. They surmise that the, further, someone’s diet is from a Western diet, the greater the variety and complexity of microbes found in their intestines. Unfortunately, these ancestral bacteria are missing from American guts. So communities in Africa, Papua New Guinea or South America, living a traditional lifestyle of high fiber plant based diet have a complex and diverse common gut microbes but these are absent in the industrialized world. The Western diet which is low in fiber and high in refined sugars is wiping out species of bacteria from our intestines. However, what was hopeful from the study was the disappearance of microbiota to undetectable levels, such as, in the gut of urban dwellers, and reappearance of gut bacteria, due to increased consumption of berries and honey, lending hope that we can enrich our microbiome by changing our dietary patterns as well. Our microbiome and us maintain a healthy symbiotic relationship and its complexity and diversity is essential for our well being, so we need to nourish it by following a proper diet.
Â
The industrialized microbiome is largely enriched with mucin-utilizing glycoside hydrolases and Verrucomicrobia, the microbiota found in mouse models deprived of dietary fiber (Nature 2017). Whereas, the Hazda and other subsistence communities have higher prevalence of Prevotellaceae, Spirochaetacea
Â
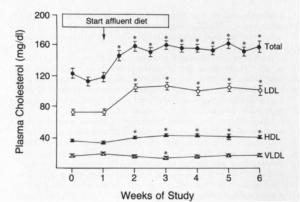
Lastly, lets learn about another tribe, which is blessed with, almost complete absence of coronary disease, the Tarahumara Indians of Mexico, who live in the high plateaus of the Sierra Madre mountains in the state of Chihuahua. They have extremely low incidence of coronary disease and cholesterol levels. They possess incredible physical stamina and are described as “modern day Spartans” and have retained ancient athletic ability unsurpassed anywhere else in the world. Tarahumara is derived from the word “Raramuri” which in their language means foot runner. For them physical fitness is essential for both sustenance and recreation. They are acclimatized to living at high altitudes in rugged terrains and their fitness challenges the current physiological concepts of maximum work load or human endurance. They are known to run up-to 100 miles in a day at a speed of 6 miles per hour. Their main diet is Pinole, a form of finely ground, toasted corn, eaten in many forms, liquid and solid. Beans provide the protein in the diet, while squash and assorted greens supply much of the carbohydrates. In times of corn shortage, wheat is used extensively and, in very lean months, numerous wild plants and roots including cactus are used including fruits. They rarely eat meat. There fat is derived from plants rather than animals. So the question, is this genetic predisposition, lack of affluence, lack of access to modern amenities, lack of sedentary lifestyle, lack of access to high calorie processed food and or lack of access to animal fats which has given rise to this super-race.  In a clever study (NEJM 1991), to answer these very questions, members of this tribe were given a high fat diet similar to our current standard american diet with significant rise of cholesterol levels within a short span of weeks providing evidence of the inherent dangers of the prevalent food consumption habits of the civilized world (Figure 6). Unfortunately, encroachment of there lifestyle with the introduction of sweets and alcohol is beginning to take its toll on this isolated tribe (Clegg, RMMJ, 1972).
 Figure 6 – Change in LDL-Cholesterol and Total Cholesterol in Tarahumara Indians on a Affluent Diet (NEJM 1991)
 Â Â Â
   
We need to understand this problem of plenty in the current world and find practical solutions. We cannot become hunter-gatherers or run 100 miles a day. But we can certainly change our diet and lifestyle to achieve health and happiness. We can walk or bike to work if possible, take stairs instead of elevators and choose whole plant based diets for better vascular health and cancer avoidance. Although difficult to achieve in industrialized nations and sedentary populations, if we adopt some aspects of their lifestyle we can potentially prevent vascular disease. Coronary atherosclerosis can be avoided if people adopt some elements of these tribes lifestyle, such as keeping their LDL cholesterol, blood pressure and blood sugar very low, not smoking and being physically active. Most of these tribes are able to live their entire life without developing any coronary atherosclerosis suggesting that lifestyle can trump genetic risk.
References:
1. Dawber et al, Framingham Cohort. Am J of Pub Health 1951.
2. Bild D et al. The Multi-Ethnic Study of Atherosclerosis. Am J Epidemiol 2002.
3. Yusuf et al. INTERHEART. Lancet 2004.
4. Lindeberg and Lundh (J Int Med 1993) – Apparent absence of stroke and ischemic heart disease in a traditional Melanesian island: a clinical study in Kitava.
5. Kaplan H, Thompson RC, and Trumble BC et al. (Lancet 2017) – Coronary atherosclerosis in indigenous South American Tsimane: a cross-sectional study.
6. Raichlen DA, Pontzer H et al. (Am J Hum Biol 2016) – Physical activity patterns and biomarkers of cardiovascular disease risk in hunter-gatherers.
8. Ong et al. (NHANES; 2007) – Prevalence of hypertension by age in the Hadza participants compared with data from the U.S.
9. Smits SA, Leach J, Sonnenburg ED et al. (Nature 2017) – Seasonal cycling in the gut microbiome of the Hadza hunter-gatherers of Tanzania.
10. Groom D. (Am Heart J 1971) – Cardiovascular observations on Tarahumara Indian runner – the modern Spartans.
11. McMurry MP, Cerqueira MT, et al. (NEJM 1991) – Changes in lipid and lipoprotein levels and body weight in Tarahumara Indians after consumption of an affluent diet.
12. Clegg R. (Rocky Mountain Medical Journal 1972) – Tarahumara Indians.
Very nice post. I just stumbled upon your blog and wanted to say that I have truly enjoyed surfing around your blog posts. In any case I’ll be subscribing to your rss feed and I hope you write again very soon!
I do believe all the concepts you’ve presented for your post.
They’re very convincing and will definitely work.
Nonetheless, the posts are very quick for novices.
Could you please prolong them a bit from subsequent time?
Thanks for the post.
Fantastic blog.Thanks Again. Really Cool.
Hi there to every , because I am truly keen of reading
this blog’s post to be updated regularly. It contains
good information.
You can definitely see your expertise within the article
you write. The arena hopes for more passionate writers such as you who are not afraid to say how they believe.
Always go after your heart.